Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 6
Open Access
Volume 6
Frederik Penzien Wainer Mamsen, MD, PhD1*; Laura Emilie Marr Spore, MD1*; Kristoffer Seem, MD2; Claes Hannibal Kiilerich, MD1; Mads Kofoed Hansen, MD3; Hannah Trøstrup, MD, PhD1,4
*Corresponding Author: Frederik Penzien Wainer Mamsen, MD, PhD & Laura Emilie Marr Spore, MD
Zealand University Hospital (SUH), Department of Plastic Surgery and Breast Surgery, 4000 Roskilde, Denmark.
Tel: (785) 766-6827, Fax: (913) 588-1660;
Email: fmam@regsj.dk; laspo@regsj.dk
Article Info
Received: Jan 08, 2026
Accepted: Jan 27, 2026
Published: Feb 03, 2026
Archived: www.jclinmedsurgery.com
Copyright: © Mamsen FPW & Spore LEM (2026).
Abstract...
Background: Non-melanoma skin cancer most commonly presents on the head and neck predominantly affecting the elder population, with surgical excision as the standard treatment. The size of the surgical defect largely determines the choice of reconstructive strategy, such as direct primary suture, skin grafts, or flaps reconstruction.
Objective: This study aims to identify predictors for postoperative complications, including hematoma, infection, dehiscence, and necrosis, following surgical excision and direct primary suturing in the facial region.
Methods and materials: Conducted as a single-centre retrospective study at Zealand University Hospital, Denmark, this study encompasses 651 patients who underwent facial surgery for Basal Cell Carcinomas (BCC) and Squamous Cell Carcinomas (SCC), all of which were closed using primary direct sutures from 2017 to 2020.
Results: The study included 499 patients with BCC and 152 with SCC, with 10.5% experiencing wound complications. A significant association was found between the risk of complications and factors such as heart disease (OR=3.72, p=0.01), consumption of more than 14 units of alcohol per week (OR=5.62, p=0.001), and multiple re-excisions (OR=8.78, p=0.03). Wound dehiscence was more prevalent in SCC surgeries (3.2% vs 9.2%). Additionally, patients with SCC exhibited a significantly higher prevalence of hypertension compared to those with BCC (p≤0.042).
Conclusion: The presence of heart disease, excessive alcohol intake, multiple local re-excisions, and the SCC subtype were linked to a heightened risk of surgical complications. No correlation between excision size, tumour location, smoking, age or diabetes and post-operative complications was reported. The study suggests considering the abovementioned factors during preoperative planning.
Keywords: Non-melanoma skin cancer; Complications after NMSC excision; Primary direct closure; Facial skin cancer.
Citation: Mamsen FPW, Spore LEM, Seem K, Kiilerich CH, Hansen MK, et al. Predictors for complications after local excision and direct primary suture in facial skin cancer: A single-centre study of 651 patients. J Clin Med Surgery. 2026; 6(1): 1223.
Introduction
Non-Melanoma Skin Cancers (NMSC) are the most prevalent malignancies worldwide, typically affecting the face and neck area, due to accumulated cellular stress from exposure to ultraviolet light, therefore primarily affect the elder population [1-4]. NMSCs are comprised of multiple dermatologic malignancies, including many subtypes with Basal Cell Carcinoma (BCC) and cutaneous Squamous Cell Carcinoma (SCC) being the most frequent. BCCs and SCC constitute 75-80% and 19% of NMCS, respectively [1,4,5]. While various therapies are available for NMSC, including radiotherapy, immunotherapy and targeted therapy, surgical excision remain the gold standard [4,6].
The goal of any surgical excision, for treatment of facial NMSC is free surgical margins [7].
Margin size is determined by factors delineating risk of recurrence such as anatomic location, size of primary lesion and histology [5]. Oncologic surgeries of the facial regions and subsequent wound closure can present a surgical obstacle due to anatomic location and aesthetic impact. Consequently, the surgeon must consider form, function and patient satisfaction, in conjunction with free margins, prior to excision. Determining whether reconstructive surgery is required or primary direct suturing will suffice rely on the combination guidelines and an individual patient assessment.
Generally, direct primary sutures are favoured for tumours of a smaller diameter, or those situated in an easy-to-excise area, particularly in cases where the surgical defect is closable with minimal tissue tension [5,8,9].
This paper aims to evaluate the indicators of wound complications, defined as those requiring intervention, following direct primary suture after the removal of NMSC from the face. We hypothesize that specific characteristics, such as age, hypertension, diabetes, as well as tumour size will
Material and methods
Patient population
This retrospective quality assurance study was approved by the Institutional Ethics Committee of Zealand Hospital, Denmark (REG-098-2020) and conducted in accordance with the Danish Data Protection Regulation.
We included all patients who underwent facial surgery for histologically confirmed basal cell carcinoma (BCC) or squamous cell carcinoma (SCC) closed with direct primary suturing at the Department of Plastic and Breast Surgery, Zealand University Hospital, Roskilde, between 1 December 2017 and 1 December 2020. The postoperative follow-up period was 12 months. Data were compiled between 1 December 2021 and 25 April 2022.
Surgical technique
Procedures were performed by Plastic Surgeons of all levels, varying from plastic surgical fellows, residents and board-certified plastic surgeons. Direct primary closure was selected when the surgical defect could be closed without excessive tension. Defect sizes were classified into four categories: 0–5 mm, 6–10 mm, 11–15 mm, and >15 mm.
Data collection
Data were extracted from electronic medical records (Sundhedsplatformen, EPIC) and entered into a standardized Research Electronic Data Capture (REDCap) database (Vanderbilt University). Recorded variables included patient demographics, surgical history, and postoperative complications, defined as surgical site infection, cellulitis, hematoma (small or large), wound dehiscence, or wound necrosis.
Duplicate or incomplete records were excluded. Data collectors followed standardized definitions and received both oral and written training. Due to patient confidentiality, the dataset is not publicly available.
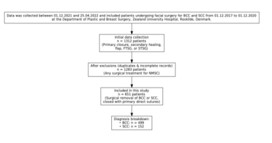
Figure 1: Flow diagram of patient inclusion and exclusion
Statistical analysis
Analyses were conducted in RStudio (R Foundation for Statistical Computing, Vienna, Austria). Logistic regression was used to assess associations between potential predictors and categorical outcome variables. Categorical data were compared using Chi-square tests. Results are presented as Odds Ratios (OR) with 95% Confidence Intervals (CI). A p-value ≤0.05 was considered statistically significant, and p-values <0.01 highly significant.
Table 1: Patient demographics.
| Variable | All, n=651 | BCC, n=499 | SCC, n=152 | p-value |
|---|---|---|---|---|
| Age, median (IQR) | 74 (66–81) | 73 (65–80) | 76 (70–82) | <0.001** |
| Male sex, n (%) | 344 (52.8) | 244 (48.9) | 100 (65.8) | <0.001** |
| BMI, mean (SD) | 25.9 (4.7) | 25.7 (4.7) | 26.6 (4.6) | 0.144 |
| Autoimmune disorder, n (%) | 56 (8.6) | 39 (7.8) | 17 (11.2) | 0.190 |
| Hypertension, n (%) | 316 (48.5) | 231 (46.3) | 85 (55.9) | 0.042* |
| Other cancer, n (%) | 124 (19.0) | 87 (17.4) | 37 (24.3) | 0.060 |
| Diabetes, n (%) | 62 (9.5) | 42 (8.4) | 20 (13.2) | 0.085 |
| Heart disease, n (%) | 245 (37.6) | 180 (36.1) | 65 (42.8) | 0.152 |
| No anticoagulant, n (%) | 368 (56.5) | 293 (58.7) | 75 (49.3) | 0.041* |
| Alcohol >14 units/week, n (%) | 55 (8.4) | 42 (8.4) | 13 (8.6) | 0.958 |
| Current smoker, n (%) | 76 (11.7) | 61 (12.2) | 15 (9.9) | 0.428 |
Results
Patient characteristics
A total of 651 patients were included in the study. The median age was 74 years (IQR: 66–81), and 52.8% were male. Hypertension was present in 48.5% of patients, and 43.5% were in anticoagulant therapy. The majority reported alcohol consumption within recommended limits, with 8.4% exceeding 14 units per week. Basal Cell Carcinoma (BCC) was the most frequent diagnosis (76.7%), while Squamous Cell Carcinoma (SCC) accounted for 23.3%.
Demographic differences between BCC and SCC patients
Patients with SCC were significantly older (median 76 vs. 73 years, p<0.001), more often male (65.8% vs. 48.9%, p<0.001), and had a higher prevalence of hypertension (55.9% vs. 46.3%, p=0.042). SCC patients were also more frequently prescribed anticoagulants (50.7% vs. 41.3%, p=0.041). There were no significant differences between BCC and SCC patients regarding BMI, alcohol intake, smoking status, diabetes, autoimmune disorders, or other malignancies (Table 1).
Tumour characteristics
The overall median tumour size was 10 mm (IQR: 6–15 mm). Approximately 47.2% had undergone previous surgery for NMSC, while 9.7% presented with local recurrence. For 281 patients (43.2%), the procedure represented their first surgical treatment for NMSC.
Postoperative complication rates
Overall, 10.5% of patients experienced wound complications following surgical direct primary suture. Most common complications included wound dehiscence (4.6%), infection (2.8%), cellulitis (1.5%), small hematoma (1.2%), necrosis (0.3%) and large hematoma (0.2%).
Figure 2 Postoperative complications after direct primary suture.
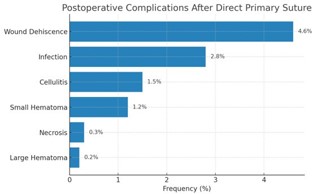
Figure 2: The figure demonstrates the percentual complications for wound dehiscence in all included patients, infection, cellulitis, small hematoma, necrosis and large hematoma.
Predictors of postoperative complications
Several independent predictors of complications related to patient demographics (Table 2). Heart disease (see supplementary table 1 for definition) was associated with a significantly increased risk of post-operative complications (OR: 3.72, p≤0.01), as was alcohol intake exceeding 14 units per week (OR: 5.62, p≤0.001), and multiple re-excisions at the same surgical site (OR: 8.78, p≤0.03). A single re-excision was not associated with a significant increased risk of complications (OR: 2.28, p=0.11).
SCC diagnosis was reported to predict a significantly increased risk of postoperative complications when compared to BCC (OR: 3.36, p≤0.01). No significant associations were found for age (OR: 0.98, p=0.2), sex (OR: 1.13, p=0.8), BMI (OR: 1.07, p=0.2), diabetes (OR: 1.18, p=0.8), autoimmune disease (OR: 1.51, p=0.5), or prior malignancy (OR: 1.10, p=0.9).
Table 2: Complications related to patient demographics.
| Demographic variable | Odds ratio | 95% confidence interval | p-value |
|---|---|---|---|
| Hypertension | 0.37 | 0.13, 1.01 | 0.06 |
| Heart disease | 3.72 | 1.35, 10.8 | 0.01** |
| No former surgery | 0.52 | 0.20, 1.28 | 0.2 |
| Local recurrence | 1.17 | 0.26, 4.32 | 0.8 |
| 1st re-excision | 2.28 | 0.79, 6.07 | 0.11 |
| Multiple re-excisions | 8.78 | 0.98, 58.3 | 0.03* |
| Smoker | 0.62 | 0.12, 2.32 | 0.5 |
| No blood thinners | 0.71 | 0.19, 3.18 | 0.6 |
| >14 units per week | 5.62 | 1.70, 18.4 | 0.001** |
| Surgery size | 0.99 | 0.92, 1.06 | 0.8 |
| Surgery type SCC | 3.36 | 1.45, 7.83 | 0.01** |
*= significant, ** = highly significant
Complication rates by tumour type
Complication rates differed between BCC and SCC (Table 3). Wound dehiscence (9.2% vs. 3.2% respectively, p=0.004) and cellulitis (3.9% vs. 0.8%, respectively, p=0.013) were significantly more common among patients with SCC compared to those with BCC. No significant differences were observed in the rates of infection, hematoma, or necrosis (Table 3).
Table 3: Complications by tumour type.
| BCC | SCC | p-value | |
|---|---|---|---|
| Surgical site size in mm, median (IQR) | 10.0 (6.0, 15.0) | 10.0(7.0, 15.0) | 0.068 |
| Surgical history | < 0.001** | ||
| Previous surgery for NMSC, n (%) | 237 (47.5) | 70 (46.1) | |
| Local recurrence of NMSC, n (%) | 59 (11.8) | 4 (2.6) | |
| No previous surgery for NMSC, n (%) | 203 (40.7) | 78 (51.3) | |
| Complications | |||
| Infection after surgery, n (%) | 12 (2.4) | 6 (3.9) | 0.394 |
| Cellulitis, n (%) | 4 (0.8) | 6 (3.9) | 0.013* |
| Hematoma | 0.163 | ||
| No hematoma, n (%) | 494 (99.0) | 148 (97.4) | |
| Small hematoma, n (%) | 4 (0.8) | 4 (2.6) | |
| Larger hematoma, n (%) | 1 (0.2) | 0 (0.0) | |
| Wound | |||
| Wound dehiscence, n (%) | 16 (3.2) | 14 (9.2) | 0.004** |
| Necrosis of wound, n (%) | 1 (0.2) | 1 (0.7) | 0.413 |
*= significant, ** = highly significant
Complication rates by tumor size and facial distribution
There was no statistically significant correlation between tumor size and complication risk (Supplementary Table 2). Distribution by anatomic region showed that BCC was significantly more common in perioral regions measuring 5–10 mm (p=0.02), while SCC was more frequent in perioral regions >10 mm (p=0.01). In the nasal region, SCC predominated among tumors ≤5 mm (p=0.01), while BCC was more frequent in the 5–10 mm category (p=0.01). In the periorbital region, BCC was significantly more common than SCC for tumors <10 mm (p=0.02 and p=0.03) (See Figure 2,3 and Supplementary Table 3).
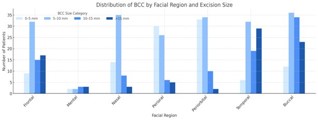
Figure 3: Distribution of BCC excisions stratified by location and size of tumour.
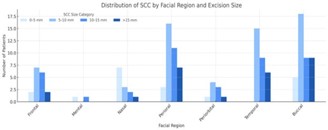
Figure 4: Distribution of SCC excisions stratified by location and size of tumour.
Discussion
This study provides an overview of demographic characteristics and wound complications following surgical excision of facial BCC and SCC with direct primary closure. While patient characteristics between the two tumour types were largely similar, patients with SCC were significantly older, more often male, and had a higher prevalence of hypertension and anticoagulant use. These findings are consistent with known age-related comorbidity patterns and gender-based prevalence of cardiovascular risk factors, rather than reflecting tumour-specific differences [0,11].
While there is extensive research on preventing surgical complications, the literature lacks comprehensive exploration of factors predicting complications following NMSC excision. Our findings indicate an overall wound dehiscence rate of 4.6% aligning with Yamamoto et al. [12]. It can be argued that complications related to wound dehiscence might, in some instances, be mitigated by opting for more advanced reconstructive techniques.
There was no difference in overall tumour size between SCCs compared to BCCs in our study (Supplementary Table 3). Even though average tumour sizes were the not significantly different between SCC and BCC, excision margin may differ since guidelines recommend different excision margins. According to the guidelines from the United Kingdom, excision of BCC; 2 cm in size necessitates a margin of 4-5 mm; however, if the tumour is located in an area where skin closure or reconstructive options are limited, an excision size of 2-3 mm may be used [13]. For low-risk SCC, guidelines suggest excision margins of 4 mm, and for high-risk SCC, excision margins should be 6mm. In our study following the Danish national guidelines BCCs are excised with a 3-5 margin and SCC with a 5-10 mm margin with some cases diverting from guidelines.
Tumor location determines end surgical technique
Interestingly, in the nasal and periorbital regions, the study found greater incidences of BCC at diameters less than 10 mm when compared to SCC. In the perioral region, we found greater incidences of SCC than BCC at diameters greater than 10 mm.
The median tumour excision size is comparable between this and our prior study [14]. Despite our prior study focusing on more complex reconstruction following NMSC excision, excision diameters may be comparable due to anatomic location of the lesions. Optimal technique for wound closure is largely driven by skin tautness, which varies widely across the facial regions, and available surrounding tissue.
Previously, an overview article has summed up how the tightness of the skin in different areas of the face should be taken into consideration when planning closure of the skin after removal of NMSC [15]. Due to the different tightness of the skin across facial regions, simple suture may be a preferable closure technique in certain areas. For example, in the frontal region, a lesion of up to 3 cm can be closed primarily with a satisfactory result, whereas perioral, if the defect is larger than a third of the length of the upper lip, local flap reconstruction should be considered over primary closure.
Clinical implications
Compared to our previous study, we found a slightly lower risk of wound dehiscence with direct primary suturing (4.6%) than with FTSG (9.2%) and local flaps (6.2%).14 A study by Homer et al. found similar low wound dehiscence after blepharoplasty of 1.4% [16]. As such, simple suture is more favourable in regard to complications than more advanced techniques when appropriate but could also reflect confounding by indication. Since there was no difference in wound complications when comparing the size of excision, we cannot propose an appropriate cut-off of excision size to delineate been simple suture and more advanced techniques.
Age versus comorbidity burden: A causal ambiguity
Although our analysis adjusted for multiple demographic and clinical variables, including age, it remains challenging to disentangle the extent to which age is an independent driver of postoperative complications, or whether it merely acts as a surrogate for a broader comorbidity burden. Patients with SCC in our cohort were significantly older and presented with more frequent hypertension, higher use of anticoagulants, and greater alcohol intake. These associations may reflect underlying differences in health status, or socio-economic factors, all of which could influence complication rates [17,18]. The study’s population was a mean of 74 years old, as the elder population around 60+ years of age is growing in Denmark the predicted patient population is estimated to increase from a total population of 1,630,370 (27.2% of population) in 2025 to 1,886,270 (30.4% of the population) [19] thereby an increase in patients and procedures will most likely increase adding to challenges that faces the public health sector [20]. However, given the established correlation between increasing age and multimorbidity, it is difficult to determine whether SCC patients are genuinely in poorer health, or whether these comorbid conditions simply co-occur with ageing. While age was not found to be a statistically significant predictor of complications, the clustering of multiple risk factors in older patients may introduce residual confounding, even in multivariable models. Furthermore, socioeconomic status and frailty—factors not captured in this dataset—may contribute to the observed differences but remain unmeasured.
This ambiguity highlights a broader challenge in retrospective observational studies: the difficulty in isolating causal relationships between closely interlinked variables. Prospective studies incorporating frailty indices, tumour staging, and patient-reported health status may provide greater clarity on whether age functions primarily as a risk modifier or a proxy for other underlying vulnerabilities.
Strengths and limitations
The main strength of this study lies in its large cohort and focus on outcomes. To our knowledge, few prior studies have reported complication rates specific to direct primary closure in facial NMSC.
A limitation of our study is that due to a lack of clear guidelines in reconstruction following NMSC excision, surgeon assessment largely drove reconstructive decisions for direct primary suturing. As a single-centre retrospective study, the findings might be subject to institutional biases and the influence of individual surgeon preferences regarding reconstructive decisions. The absence of radiotherapy history in our database is also a limitation, as prior radiation can significantly impact tissue quality and wound healing. Furthermore, the study did not differentiate between junior plastic surgical residents and board-certified plastic surgeons, which could introduce variability in surgical technique.
Conclusion
This present study concludes that the risk of wound complications is low in both BCC and SCC after removal and direct primary suture in the face. Excision size is not associated with increased risk of post-operative complications. On the contrary heart disease, alcohol intake above recommended limits and several local re-excisions increased the risk of complications. The observation that cardiovascular disease, alcohol use, and repeated surgical interventions were associated with higher complication rates is consistent with clinical reasoning. Yet, it is somewhat unexpected that conditions known to compromise wound healing—such as diabetes, immunotherapy, and smoking—did not appear to significantly impact outcomes in this cohort. This challenges assumptions and highlights the need for a more nuanced understanding of risk stratification in facial reconstructive oncology.
Future research directions
Further work is necessary to determine scientifically based decision-making between direct primary suturing versus more advanced techniques for skin closure after removal of NMSC in the various facial regions. This work must ideally attempt to randomise simple suture vs flap or FTSG in specific facial subunits to eliminate individual surgeon preference and anatomical variance.
Declarations
Author contributions: Conceptualization, FPWM, CHK and HT; methodology, FPWM, KS, CHK, HT; software, FPWM, LEMS, CHK; validation, FPWM, KS, LEMS, CHK, AG and HT; formal analysis, FPWM, CHK and HT.; investigation, FPWM, KS, LEMS, CHK, AG and HT; resources, HT; data curation, FPWM and CHK; writing—original draft preparation, FPWM and KS.; writing— review and editing, LEMS and FPWM; visualization, FPWM, LEMS, CHK; supervision, FPWM and HT; project administration, FPWM and CHK; funding acquisition, HT. All authors have read and agreed to the published version of the manuscript.
References
- Urban K, Mehrmal S, Uppal P, Giesey RL, et al. The global burden of skin cancer: a longitudinal analysis from the Global Burden of Disease Study, 1990–2017. JAAD Int. 2021; 2: 98–108.
- Katalinic A, Kunze U, Schäfer T. Epidemiology of cutaneous melanoma and non-melanoma skin cancer in SchleswigHolstein, Germany: incidence, clinical subtypes, tumour stages and localization (epidemiology of skin cancer). Br J Dermatol. 2003; 149: 1200–1206.
- Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol. 2012; 166: 1069–1080.
- Rampinelli V, Pinacoli A, Piazza C. Head and neck nonmelanoma skin cancers: surgical management and debated issues. Curr Opin Otolaryngol Head Neck Surg. 2024; 32: 62–70.
- Badash I, Shauly O, Lui CG, Gould DJ, et al. Nonmelanoma facial skin cancer: a review of diagnostic strategies, surgical treatment, and reconstructive techniques. Clin Med Insights Ear Nose Throat. 2019; 12: 1–10.
- Villani A, Potestio L, Fabbrocini G, Scalvenzi M. New emerging treatment options for advanced basal cell carcinoma and squamous cell carcinoma. Adv Ther. 2022; 39: 1164–1178.
- Lane JE, Kent DE. Surgical margins in the treatment of nonmelanoma skin cancer and Mohs micrographic surgery. Curr Surg. 2005; 62: 518–526.
- Linares F, Iglesias ME, Martínez-Amo JL, Cabo F, Tercedor J, et al. Reconstruction techniques of choice for the facial cosmetic units. Actas Dermo-Sifiliográficas Engl Ed. 2017; 108: 729–737.
- Eskiizmir G, Cingi C. Nonmelanoma skin cancer of the head and neck. Facial Plast Surg Clin N Am. 2012; 20: 415–423.
- Connelly PJ, Currie G, Delles C. Sex differences in the prevalence, outcomes and management of hypertension. Curr Hypertens Rep. 2022; 24: 185–192.
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023; 147: E93–E621.
- Yamamoto R, Homma K, Masuzawa Y, Shimizu C, et al. Early complications following facial laceration repair performed by emergency physicians after one year of wound closure training. AEM Educ Train. 2018; 2: 259–268.
- Newlands C, Currie R, Memon A, Whitaker S, et al. Non-melanoma skin cancer: United Kingdom national multidisciplinary guidelines. J Laryngol Otol. 2016; 130: S125–S132.
- Mamsen FPW, Kiilerich CH, Hesselfeldt-Nielsen J, Saltvig I, et al. Risk stratification of local flaps and skin grafting in skin cancerrelated facial reconstruction: a retrospective single-center study of 607 patients. J Pers Med. 2022; 12: 1–10.
- Erkul E, Patel KG, Day T. Surgical planning for resection and reconstruction of facial cutaneous malignancies. Int J Head Neck Surg. 2016; 7: 149–164.
- Homer NA, Zhou S, Watson AH, Durairaj VD, et al. Wound dehiscence following upper blepharoplasty: a review of 2,376 cases. Ophthalmic Plast Reconstr Surg. 2021; 37: S66–S69.
- Britteon P, Cullum N, Sutton M. Association between psychological health and wound complications after surgery. Br J Surg. 2017; 104: 769–776.
- Fayne RA, Borda LJ, Egger AN, Tomic-Canic M. The potential impact of social genomics on wound healing. Adv Wound Care. 2020; 9: 325–331.
- Danish Statistical Institute. Population projection 2025 for the entire country by origin, sex and age. Copenhagen: Danish Statistical Institute; 2025. Available from: https:// www.dst.dk/da/Statistik/emner/borgere/befolkning/ befolkningsfremskrivning
- Schmidt M, Schmidt SAJ, Adelborg K, Sundbøll J, Laugesen K, Ehrenstein V, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019; 11: 563–591.